

Employer Dilemma: A Framework for Returning to Work [ Safely ]
We are fortunate to work with some of the largest employers in the country, most of which have followed local or federal guidelines and ceased operations in the workplace because of COVID-19. They had to do this with little opportunity to reflect on the impact or prepare for an eventual transition back to the workplace. Now, eight weeks later, many are anxious to find ways to bring employees back but face a tough dilemma—how do they do so safely?
With little hard information on the post-pandemic future, executive leadership must still answer to shareholders and stock prices, and those serving in the health and wellness areas of companies are being thrust into an equally precarious position. While “Returning to Work” may seem like a straightforward task, it is anything but. Facility Managers, EH&S leaders, and Health Benefits leadership are being asked to safely and effectively return their populations despite uncertainty, risk, and potentially serious consequences—for their business and for skeptical and worried employees alike.
The decisions being made by Human Resource and Facility leaders are forcing them to step far beyond their training and experience to scope out policies, procedures, and approaches to accomplish the Return to Work safely mandate. These leaders are effectively getting crash courses in population health, contact tracing, interior design that is “safe sixed,” environmental safety, closed room flow dynamics, and a host of other pandemic-related topics. When global leaders in politics and health can’t yet agree on the best approach, it is a certainty that leaders of companies will also struggle with this task. In such a scenario, what everyone is looking for is common sense from trusted advisors who can provide practical guidance and appropriate medical advice that is timely, relevant, and can be incorporated into a variety of Return to Work safely approaches.
RETURN TO WORK FRAMEWORK
The purpose of this post is to share with clients and others the key components of what we believe should be included in any Return to Work safely conversations. We realize that many of our employers are actively involved with numerous initiatives on their own, but it can be challenging to bring all of these together into a coherent strategy. We believe that we can contribute in a multitude of ways—from serving as the trusted advisor to actually implementing the entire framework as part of that coordinated approach. In any situation, we want to be most useful to each client based on the resources we can bring together in partnership. And I hope what we learn alongside our clients can be applied to other companies struggling to be decisive despite dilemmas related to their own Return to Work strategy.
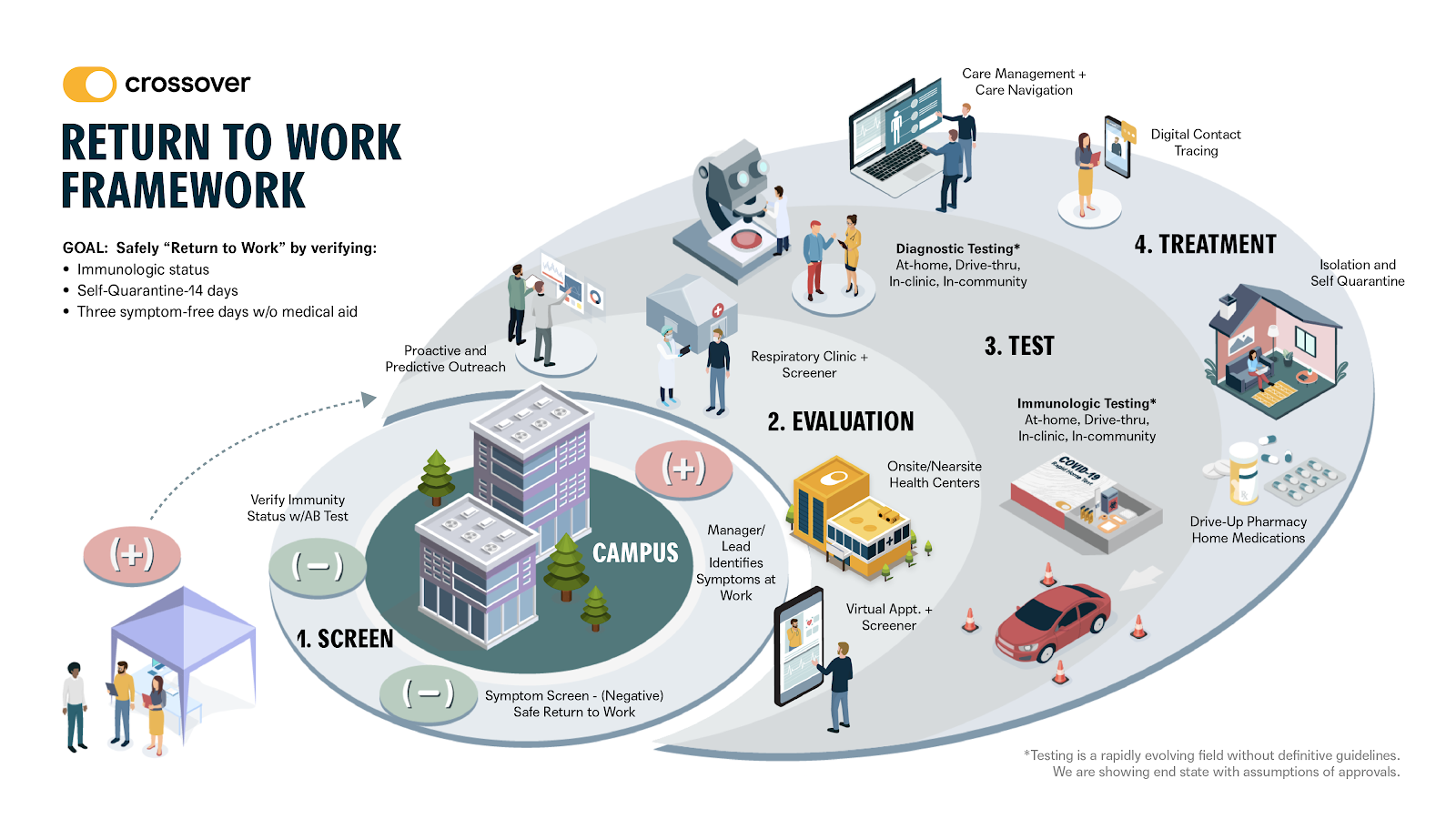
There are four key elements in our proposed framework:
- Screen. The ability to actively screen employees is the first line of defense. Screening can come in the form of temperature checks/scanning as well as through a screening questionnaire or other electronic attestations. Individuals with verified immunologic status or confirmed negative screenings are allowed onto campus. If the individual manifests positive symptoms before entering the campus or develops these once there, he or she is immediately sent for evaluation.
- Evaluate. The evaluation of employees who screen positive can take several forms based on the capabilities of the campus. These options include: “Symptom Clinics” where patients are triaged in settings removed or isolate from the rest of campus; the Health Center (either onsite or nearsite) to evaluate employees with symptoms; or a virtual appointment with built-in screeners. We also see a role for predictive analytics to identify patients who are at risk for COVID-19 and that we can proactively reach out to evaluate prior to arriving back on campus or as needed at the earliest sign of symptoms (potentially via wearable devices).
- Test. On the testing front, we separate out Diagnostic versus ImmunityTesting. Diagnostic Testing has multiple channels, including those that can be done in center, in community, via a drive thru, and also new tests that are being approved for home use. All of these tests are intended to evaluate the presence of active infection and have specificity/sensitivities based on the activity level of the virus. Repeat testing is recommended and often required. Immunity Testing represents the other end of the continuum in that they measure the presence of antibodies, and can give a sense of the recency of infection, presence of immunity, and prevalence in the community. These also can be delivered via home use, via drive thru, in clinic and in community. We believe that a robust antibody testing program completed remotely at home, but overseen by a virtual care team (physician administered rapid testing), is the most promising testing methodology to achieve the scale required to meaningfully return large number of employees back to campus. As we often say, we believe proof of serological immunity will become the new employee badge.
- Treat. If an individual has been diagnosed with active disease, there are multiple treatment options including isolation, symptomatic care, and any associated care management or care navigation services that may be needed. Surrounding employees with a full care team can be enormously reassuring for patients who test positive. This is an outcome of our “COVID Care” experience whereby we leverage our already established relationships and connectivity to ensure members have what they need, can be directed to additional resources as necessary, and have someone walking with them as they progress through the infection.
WHAT THIS MEANS FOR EMPLOYERS IN GENERAL
Our perspective is that most employers are being thrust into a population health arena where they have no experience, no training, and are feeling quite unprepared. Our Medical Group can significantly ease these concerns by offering sound counsel and advice to support the clinical decisions, policy approaches, and treatment validations that need to be made to balance clinical, public, and corporate safety issues. This is what we call our Chief Medical Officer “as a Service” (in which we lend our medical expertise in an outsourced way to all of our employer clients). This specific offering has been part of our overall population health services that employers justifiably have never had to consider before.
As we all move forward in addressing the pandemic and our return to work, there will be many who come forward to help. Crossover wants to be clear about the attributes which enable us to meaningfully contribute through our unique value proposition:
- We are a “National” Medical Group with licenses in 50 states to serve employer populations.
- Our virtual care teams can order tests, review results, prescribe treatments, organize care management plans, provide care navigation, plug employees into employer-offered programs, and generally surround members with our tech, our teams, and our high-touch service.
- We are at our best when we are assigned a defined population, served by a designated care team, with our patient-members surrounded by our comprehensive care model adapted to service pandemic primary care needs (as described previously).
- We can guide employers to a financial model that makes sense both for comprehensive primary care services, as well as adjustments that include pandemic-only services. This includes shorter term contracts, limited services, and ultimately it must include an at-risk model when we are embedded in longer term relationships.
At the end of the day, primary care has a vital role to play both in a pandemic and as well as helping companies emerge safely on the other side. Crossover is already well-positioned as a trusted advisor to provide general guidance, but now more than ever, our value as a medical group that can also execute these programs is a key differentiator. The assets and capabilities of our primary care model are easily adaptable and can flex to meet emerging needs like pandemic primary care, testing and monitoring, future testing/policies/practices, and more. And for our employer partners being thrust into these uncharted population health dilemmas, we can help them deliver and return everyone safely to work!


Leave a Reply