

The Great Consolidation, Part 3: The Three Organizing Categories for Employer Health Services
The Great Consolidation series is an attempt to articulate my views on how the exploding numbers of digital health apps, as well as growing number of companies claiming to be Full Stack health platforms, will begin to coalesce around a few leaders. My particular focus remains on the Employer Health space, but the trend applies across virtually all of the digital health industry including all forms of secondary care services that touch health systems, specialists, diagnostics, imaging, and related facilities. Part 1 focused on describing the Great Consolidation by using other technical innovations that represent analogous prototypes for what we can anticipate for healthcare. Part 2 highlighted the capabilities that will characterize the various “winners” in the space—effectively creating a self-reinforcing, virtuous cycle of technology-enabled and human-powered innovation. In Part 3, I am highlighting how the various approaches will gravitate around one of three organizing categories, and I’ll predict which category will ultimately become the most compelling and why (Part 4).
I find the organizing the various vendors and players in the market into three categories is useful. These categories represent different ways to respond to the many challenges faced by employers in managing an increasingly complex health benefits environment. This includes the frustration of managing multiple disconnected vendors, as well as the maddening issue of integrating the various offerings, different procurement cycles, conflicting marketing efforts, and an ecosystem generally run amok. Each of these categories is a natural evolution of the technology and service offerings as well as a convenient way to think about the problems each approach attempts to solve—better data for better decisions, better tech for better coordination, or better care for better outcomes. Solving for the Triple Aim (cost, quality, and experience) is no joke, and you wouldn’t expect a cheap punchline to be the answer to this very difficult problem.

So let’s look at each category approach in turn:
The Navigation solutions are predicated on the idea that the greatest barrier to meeting the Triple Aim is the complexity of both a patient’s care journey as well as the confusing benefit offerings from employers. Care Navigation serves both concierge (holding members’ hands through the referral process) and gatekeeper (curating technology point solutions as well as the entire range of secondary care services including specialists) functions. The seamless relationship between Patient and Navigator and then Navigator back to Employer/Payer is the key to making this work within the thesis that navigation can remove friction while making better connections. Some of the curation and handholding will be human-powered, but in order to scale, the majority must be automated over time. Navigation can be effective but always bumps up against the inability (or willingness?) to go “far enough” into an increasingly blurry line of care delivery.
The Technology solutions represent a more classic IT strategy, creating an all-in “operating system” for all of its participants: patients, providers, and payers. A large number of the recent digital health acquisitions involve companies looking to build enough capabilities to begin to fulfil their Full Stack ambitions. This often reflects a company’s desire to expand from “just” technology to cracking into new services (or the other way around), as well as broadening the scope of those services to more effectively compete as the landscape shifts. The end game here is to create a digital, walled garden, where value (ease of use, expanding services, efficiency of coordination) becomes a network effect in and of itself. Taking an operating system approach implies you are a foundational part of how something works, but it may also pigeonhole you into a commodity infrastructure and thereby subject you to an inevitable “race to zero” (i.e., telehealth or virtual care is effectively—rightly or wrongly—perceived as a commodity).
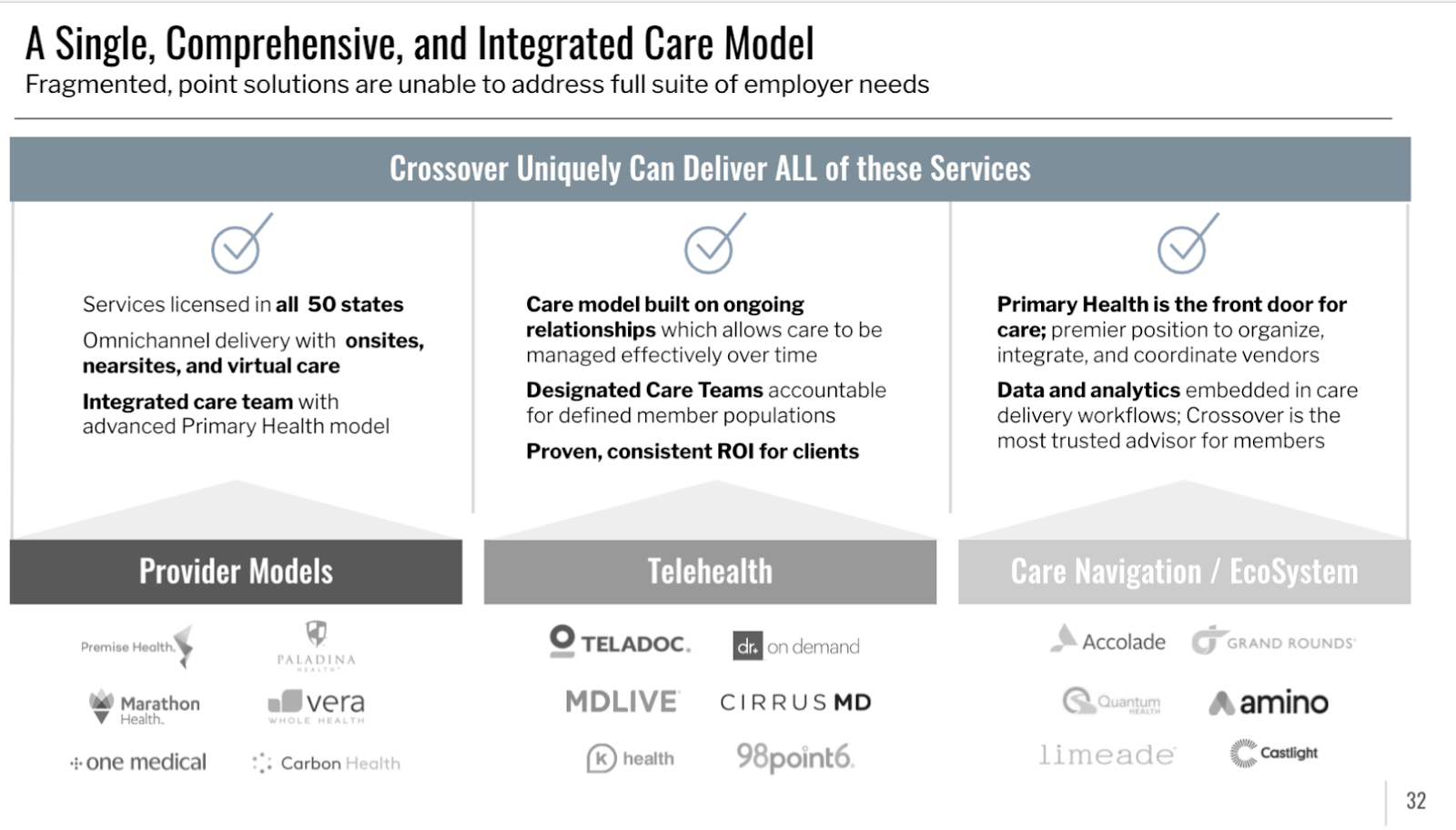
The Care category as delivered by a national Medical Group is a new and emerging option for health activist employers to organize their employer’s ecosystem. Historically, there hasn’t been a medical group with a strong enough gravitational pull to organize the constellation of vendors in the employer orbit. Medical groups have instead chosen to be part of the network apparatus of the health plan—a provider “node” on the greater insurance “network.” However, with the advent of direct practice mirroring the trend of direct contracting, a new category has begun to evolve. This requires a medical group to be facile with data, able to develop integrating technology, have native product capabilities, orient around membership, have legit marketing and engagement skills, and enough moxy and gravitas to convince benefits leaders that there is in fact a third option. What’s even better is that a technology-enabled medical group removes a key integration point where the connection often gets dropped. When the medical group can coordinate and deliver the care, when we can recommend and complete the referral, and when we can advise and be accountable for the outcome—that becomes truly powerful.
Perhaps, the best question to ask in an era of consolidation may be—is it better to be a medical group that becomes more technically enabled, or is it better to be a technology company bolting on care as if it were fungible? Is your entire company architected for care and caring, or is it built for speed and scale? Or…can it be both?
At Crossover, we have been focused on building a scalable, national network of employer-based care from the beginning. Not only have we embraced the four capabilities required to deliver on the Triple Aim, but we are now offering a “third space” for employers to organize care delivery. Our Full Stack vision means that we see a world in which we either develop the capabilities ourselves or embed partner organizations deeply into our vetted care pathways. This also means that employers get the integration, the reporting, simplified procurement, and the coordination inherent within our accountable care model.
Our Full Stack Primary Health offering enables a simplified, comprehensive member experience that spans the entire primary health journey. For the first time, another option is available that provides employers an alternative organizing category. But there is one final element that will ultimately matter most in the Great Consolidation. And, that will be the focus of the final chapter of this series.


Leave a Reply