

Clarity through Contrast: The Crossover Couplet
In the race to meet rapidly evolving care needs, there has been a Cambrian explosion of innovation in the digital health and virtual care* space. Both in practical application and in theory for some, these advancements are designed to create more access, lower costs, simplify complex workflows, and address niche market needs. As welcome as many of these new offerings are, however, I have also noticed a trend that isn’t as beneficial to the member nor the ultimate payer of these services: the lumping together of all of the various solutions into one amalgamation, when in fact, the clinical capability and value of each solution is very different. Chatting online with a random gig physician about pink eye is very different from working with your dedicated, integrated care team as they manage complex, ongoing health issues. They are not comparable—and undiscerning purchasers are always susceptible to incongruent math of “all this for $1 PEPM.” In short, the employer or health plan evaluating the solution needs to ask the right questions to understand where quality and outcomes come to play when evaluating cost.
To help create differentiation and distance in the various care delivery approaches, Crossover has achieved clarity with clients by sharing the following contrasting couplet:
“Care is care…but care is not fungible.”
Let me explain:
“Care is care…
In 2020, the pandemic pretty much pushed everyone to virtual care. Because Crossover already had established, in-person relationships with our members, we clicked seamlessly to virtual when physical access was not possible. In an environment where so much care was deferred, we found that our members carried on almost as they had before the pandemic. In fact, the last 16 months confirmed our thesis from June 29, 2019, that 70% of our care could be delivered virtually:
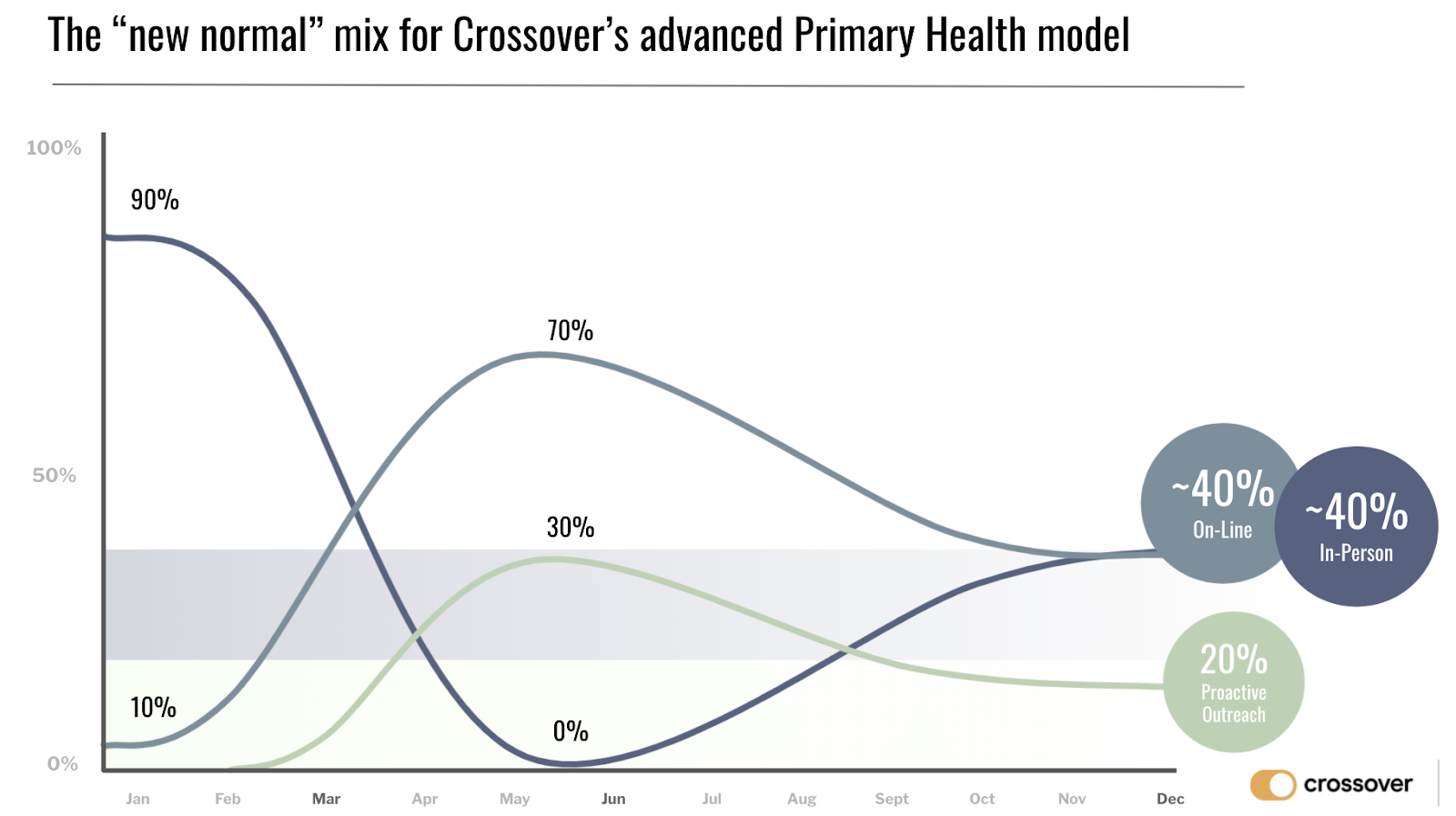
In our unique omni-channel offering, our members—again, given their existing relationships with our care teams—realized that they could receive quality care regardless of the care channel. At Crossover, “Care is Care” (wherever and whenever it was experienced) became not just a catch phrase, but a calling card to both members and care teams who now could see clearly the advantages of the multi-channel approach. Based on our internal metrics we could see that members felt omni-channel, relationship-based care — whether in person or online — also meant quality, results-driven care. We saw this fundamental shift occur throughout the pandemic and it has continued to be the case as we enter the back half of 2021. While the general healthcare world continues hypothesizing about “care in a post-COVID world,” we’re already operationalizing this brave new world of care.
…but care is not fungible.”
While the member experience should be high quality regardless of the care channel through which it is delivered – care cannot be evaluated just by a single interaction. What has now become clear in the market is that the pandemic pushed people TO virtual care, but it will also push them THRU what many found to be very thin “urgent care only” offerings. While the pandemic played a significant role in legitimizing virtual care, COVID as a medical condition also highlighted the many facets of managing a chronic health condition including how care needs evolve over time. Conditions like COVID are best managed through longitudinal relationships with an accountable medical partner. Primary Health, as offered by Crossover, is something functionally and categorically different. The level of care is NOT fungible, or equivalent, let alone substitutable, across these different solutions. The Emperor, as they say, may really be wearing pajamas!

Your gig urgent care physician versus your fully dressed and fully integrated clinical care team doesn’t compare.
History doesn’t repeat itself, but it often rhymes
My prediction is that the active rush of vendors into virtual care will be met with an equally reactive push back to solutions that deliver real care from actual, tech-enabled humans (sorry chatbots!) that are true experts at managing health. Crossover’s care model cannot be compared to nor priced equivalently to these lighter, thinner, and less satisfying substitutes. The really meaty value-based outcomes are best achieved by an integrated, coordinated, and comprehensive care model. Remember, you can’t impact healthcare cost without directly taking on healthcare delivery. And, while “care is care… ” for care models based on an ongoing relationship, the absence of a relationship implies by definition that all “…care is not fungible” as well.
The Crossover Couplet perfectly describes our care model as “poetry” in motion!
*Both “Digital Health” and “Virtual Care” are seemingly interchangeable terms that lack specificity. They’re used to describe telemedicine, telephonic, asynchronous, and other forms of “digital” delivery of care which creates unnecessary confusion as well as a lack of clarity. The Crossover Couplet was created to illuminate and eliminate this opacity.


Leave a Reply