

Origin Story: How Members Flow between Services and Channels
The American Telemedicine Association Annual Conference & Expo (ATA 2023) kicked off this past weekend in San Antonio. Crossover has a strong presence at ATA this year in a thought leadership role (see blog posts by the head of our virtual practice, Danna Chung, MD and o-founder Nate Murray on our hybrid care delivery model, as well as presentations by Yvonne Hawkins, MD and Matt Debole, DPT). Over the years, ATA has appropriately moved its focus away from the technology of telehealth toward care that can be enabled through this delivery channel. This transition is consistent with the recent Rock Health study looking at the post-pandemic adoption rate of digital health services and tools, which is now approaching 80%. While the article appropriately highlights this adoption as occurring at “the speed of trust,” the subtext is that the explosion of digital health solutions has, unfortunately, replicated much of the fragmentation, disconnection, and frustration for patients of the in-person experience.
Our goal at Crossover is to bring more continuity and coherence to virtual care, not just as a technology, but, more importantly, as a vital part of the care delivery model. We believe not only that adoption will continue to increase linearly, but also that virtual care’s impact and efficacy can increase exponentially when digitally-delivered services are embedded into comprehensive primary health models (ie, interdisciplinary team-based care model built on trusted, longitudinal relationships with a focus on outcomes). We believe that smoothing how the member “flows” between in-person and online services by increasing the fluidity of connection will be a key catalyst.
This ties to the broader issue of member “flow” and how it relates to my ambition to displace the “visit” as the sole indicator of value in primary care. The idea of member flow is not intended to describe the member journey nor the care team clinical workflows. Instead, it describes how a member utilizes and experiences an integrated, multi-channel care delivery model. In other words, how easy is it for a member to flow between care services (different disciplines) and across care channels (from in-person to virtual)? From this perspective, and in the spirit of using the timing of the ATA Annual Conference to highlight emerging patterns of care, I thought it would be helpful to share some early insights into how Crossover’s continuous care model (aka “streaming care”) actually performs.
Flow in Context
For some basic background and statistics to provide the context: Crossover offers an integrated care delivery model called Primary Health, which is inclusive of primary care, mental health, physical medicine (physical therapy, chiropractic, and, in some locations, acupuncture), health coaching, and care navigation. Members can be seen by any of the service providers without any barriers—i.e. they can book directly with primary care or health coaching—and as in other value-based care models, our providers have no incentive other than the provision of good care when referring to the other service lines.
To better understand member flow, we reviewed the data in several steps with our data science team. First, we found that of individuals who used any of Crossover’s service lines in 2022, just over 80% say that Crossover is their primary way to receive care. Second, of those who use our services, 74% use primary care, 20% use physical medicine, 10% use mental health, and 7% use health coaching. Third, we took an all-time, cross-sectional sample of over 180,000 members who had engaged with primary care first and then went onto another service. Finally, we did the opposite by reviewing members who started with a non-primary care service to see how often they then later received a primary care visit (each between 15k to 50k engagements depending on the service line evaluated).
So, within this setting of member choice and provider autonomy to make the best clinical decisions, how do members “flow” through Crossover?

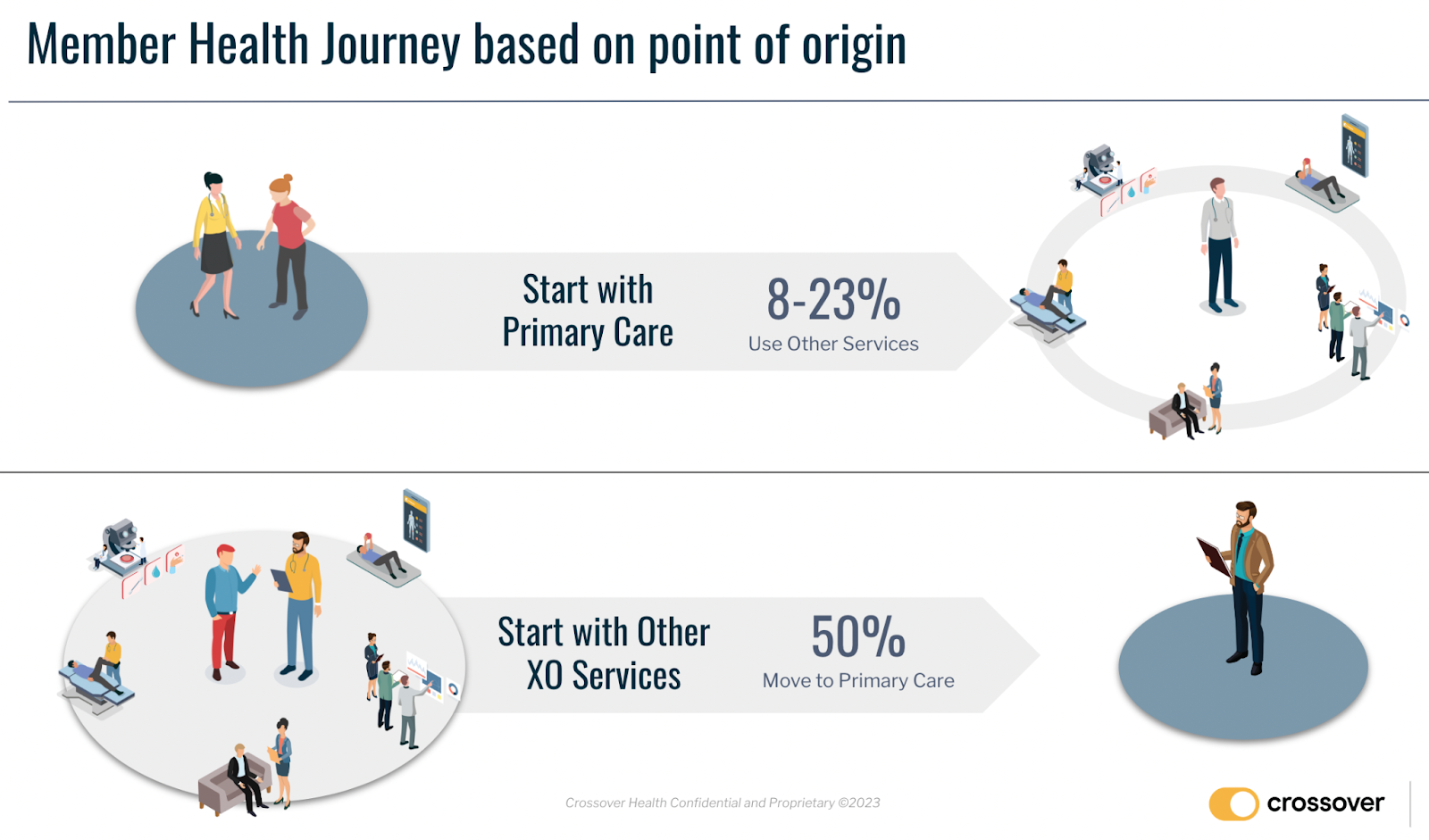
It turns out that there is a big difference in member flow depending on where a member starts their care journey. If primary care is the origin service, he or she is referred to another internal service about 8-23% of the time. If a member starts in another internal service, he or she is referred back into primary care about 50% of the time. As noted previously, there is no financial or clinical incentive to refer one way or the other or at all. Therefore, we assume these are natural patterns based on both member and provider choice and collaboration in achieving best outcomes.
Flow Findings
It is clear that primary care is a driver for members to engage in their health. Most people who start with primary care get their annual basic screenings completed, preventive care reviewed, and chronic conditions addressed. From this origin point, they are referred as needed to our other services. This pattern is likely heavily influenced by the underlying health of our commercially insured population in the employer health setting. Both preventive and problem focused visits appear to generate the need to refer to our other services between 8-23% of the time and we also refer out to third-party specialist about 12.5% of the time as well.
Arguably, the flow works even better the other way around. If members engage with our other services first, they end up seeing our primary care providers just under 50% of the time. We believe this is because members have a great experience with their ancillary provider, prevention is highlighted, and both contribute to the motivation to establish a care relationship via primary care. Every service line directly addresses prevention, screening, and social determinants of health, by design. If a member comes in for a mental health or physical therapy issue, our screenings can identify other health concerns that may also need to be addressed. That chronic back pain a member is experiencing may prompt him or her to reestablish a care baseline with a primary care visit that can be flexibly delivered either in person or online.
This data is vital to us. When providing Advanced Primary Health—with its multidisciplinary care teams and continuity of access, relationships, and data—member “flow” is a much more relevant concept than a single member “visit” in isolation. We want to ensure that for every member, each touch point is a catalyst to help him or her flow along the health journey, unfettered by professional silos, complex payments, or gaps in data and care continuity. We believe that if our members can embrace all aspects of our model, then they can better make the commitment to embrace all aspects of their health to the care team that has earned their trust through time, attention, and a focus on flow.


Leave a Reply