

From Hype to Hybrid: Choice Architecture in Care Access
My last post referenced an NEJM article which spoke about the challenge (impossibility?) of reconciling new care delivery models with fee-for-service compensation. Hot on the heels of this is our release of “From Hype to Hybrid”—a summary of Crossover research results authored by our Chief Medical Officer, Stephen Ezeji-Okeye, MD. The paper shows that, when the innovation-stifling overhang of fee-for-service is removed, the natural state of how our members use our services evolves to a new equilibrium of hybrid care. It varies by discipline, but at the end of the day, the members are in the driver’s seat—what an amazing concept (only within healthcare)!
We would argue “Hybrid” should be the word of the year as a result of the great experiment forced upon us by the pandemic. There is, however, a generally unsophisticated and limited understanding of what hybrid means in practice and potential. In commercial real estate, for example, hybrid work simply means the option to work “at the office” or “from the home.” This binary understanding misses the much richer opportunity companies have to redefine how, when, and why people should get together, what kind of physical and virtual spaces they need for efficiency and productivity, or, what corporate hierarchy even looks like (many companies are moving to no headquarters). And, as companies are starting to see, not offering the choice or not investing in the management systems vital to this evolving approach to work is costing them in terms of employee engagement, productivity, and retention.
It’s analogous in healthcare, and especially, Primary Health. As we all know, the pandemic made online primary care mandatory. But as restrictions have eased, more members in traditional healhcare are returning to in-person visits, reducing the percentage of virtual care often dramatically. Is that members’ choice, or has it been forced on them, in particular by the fee-for-service regime and the systems it fosters?
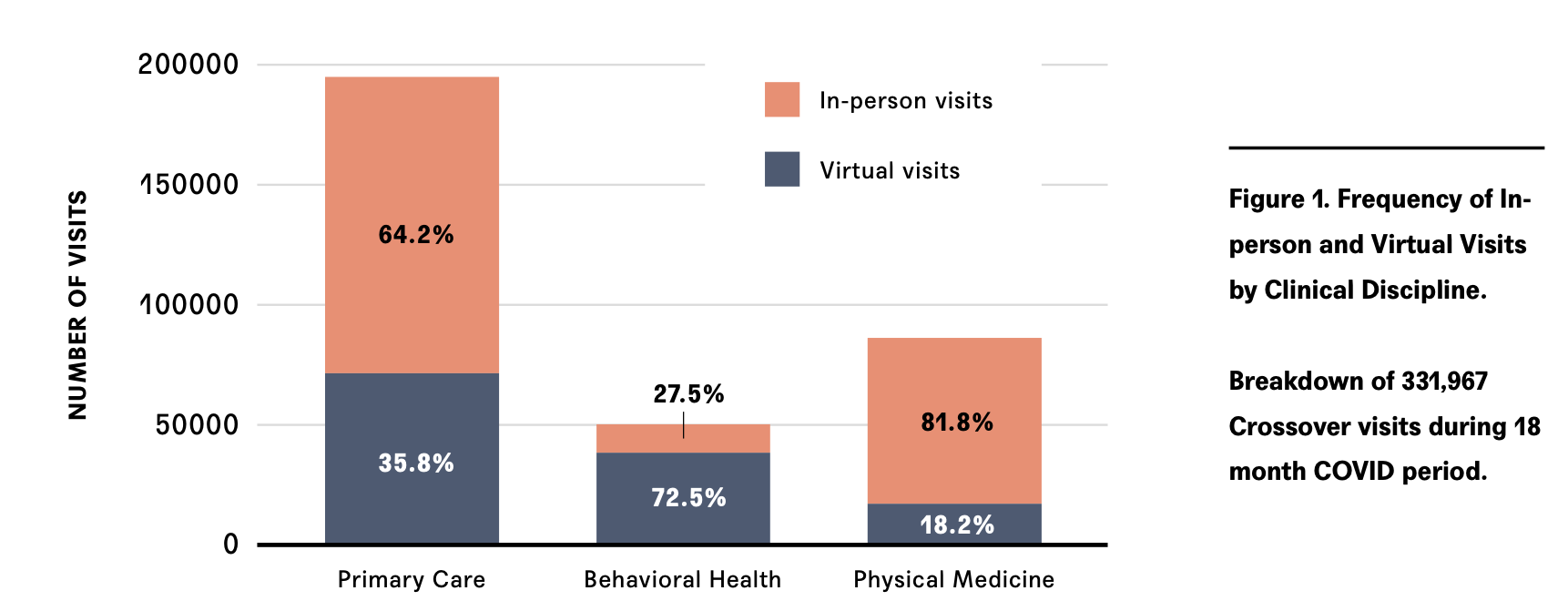
Stephen’s research in “From Hype to Hybrid” suggests the latter. As we do not engage in fee-for-service at Crossover, we are not bound to volume, transactions, or coding—we are guided only by outcomes. This means we don’t coerce, nor really have a preference for, what channel the members choose to see us. If a member’s health journey is best accommodated by in person so be it. If we can appropriately guide them to virtual so be it. If we need to include other members of the care team (our paper highlights the collaboration between primary care and physical therapy) then so be it. The result is that Crossover has—over almost 350,000 encounters—seen the use of virtual channels range from about 20% in physical medicine, to 33% in primary care, to almost 75% in mental health. And we expect these numbers to continue to evolve upwards as members get more comfortable with the range, possibilities, and ease of newer forms of virtual care.
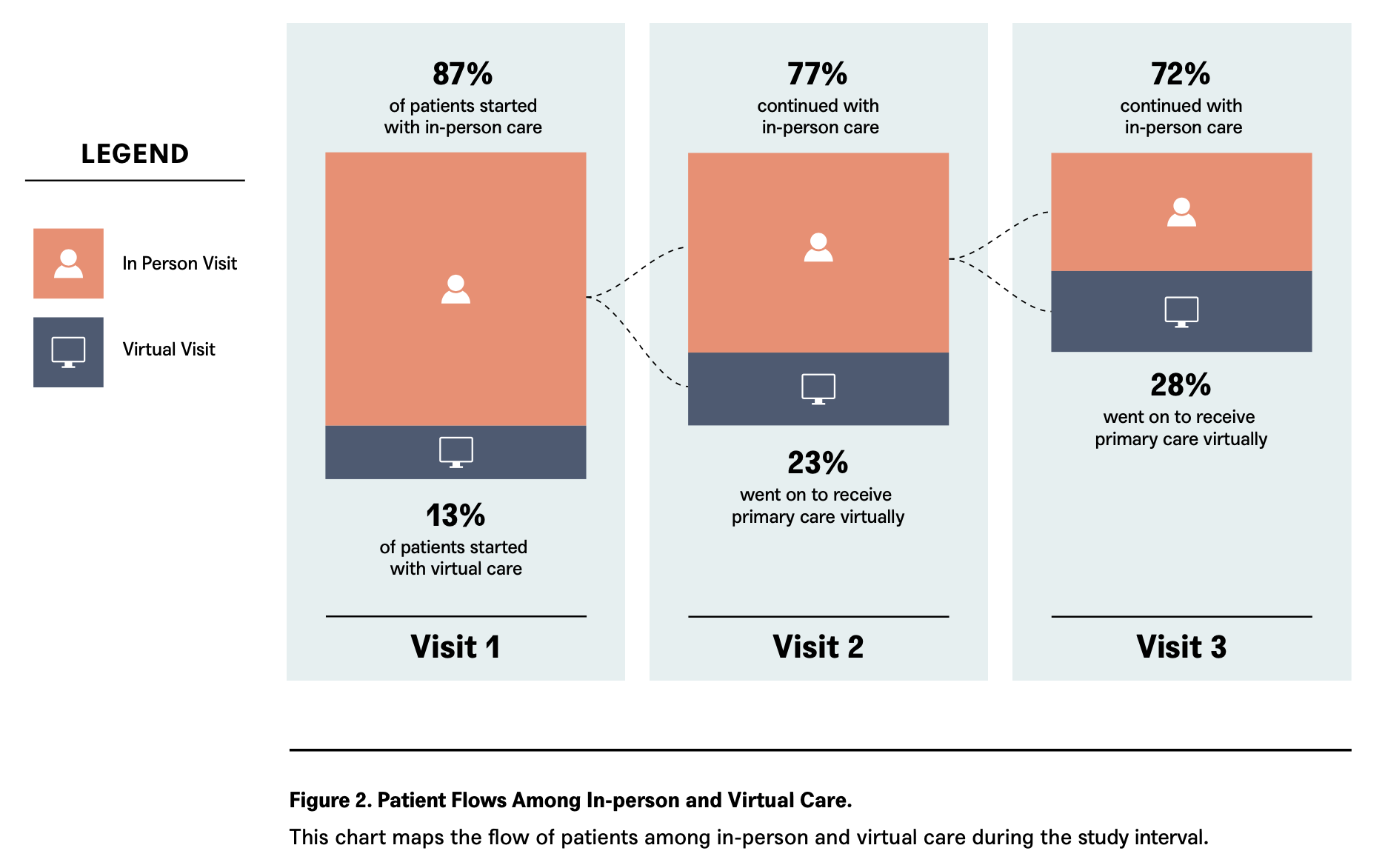
One thing that’s fascinating about the research is how it shows members organically flowing from one channel to another through the course of their Crossover experience. It shows that the amount of virtual engagement increases with more visits—this suggests that the promised efficiency and effectiveness of virtual care is being realized naturally as part of the course of the ongoing provider/member relationship. As we see it, this recognition is inevitable as members learn that each medium has its advantages at different points along their journeys, and that our model gives them the choice.
However, just as companies need to evolve management practices to ensure the hybrid offering moves beyond “work at the office/work from home,” the choice offered by medical providers needs a genuine rethinking of the systems that support it. For us, team-based care, at the heart of our Primary Health model, is the main lever, but the support system also needs flawless communication, engaging experiences online and in person, and a deep understanding from our employer partners that the apparent open-endedness of our model will lead to lower costs, as well as better outcomes, and happier members. Measuring the number of visits may be a familiar metric, but it’s not the right one in a choice-driven, technology-enabled world.
Creating this type of choice architecture doesn’t come as part of some bolt-on, patchwork process. It requires a fundamental redesign and rethinking of existing models, which calls into question the viability of services and platforms that are rooted in one channel (be that physical or digital) as well as in legacy compensation models. Members will absolutely need primary care models that are purpose built to meet them wherever they are while also driving the tangible and objective health outcomes that matter .Stephen summed it up best in his conclusion:
Choice architecture that leads to a great clinical destiny!


Leave a Reply