

Hard Work—The Climb to a Value Based World
We have been talking for a long time about the fundamental role payment architecture plays in the destiny of how care is delivered, experienced, and how it performs. While most people in the industry would agree that the current fee for service payment model is a root cause contributor, there seems to be only scattered efforts to make the full transition to value-based care (ChenMed, Aledade, etc.). Even in our own industry—employer health—there is much talk about value-based care, but there has been limited movement to pursue this strategy at scale (again, there are a few notable exceptions, including Cisco). While the view of a fully transformed health system is beautiful from the mountain top, it is unfortunately still a pretty remote and isolated place, summited only after an incredibly arduous climb.
This is why my interest was piqued from a recent New England Journal of Medicine article written by Julia Adler-Milstein, PhD (Director of the Center for Clinical Informatics and Improvement Research at UCSF) and Ateev Mehrotra, MD (Harvard Medical School) describing the challenges of coding and getting reimbursed for new digital health services. While the pandemic accelerated the use of virtual care as well as several new care delivery approaches, it also brought the issue of paying for these new innovations with old models front and center to be exposed to the glaring spotlight. In fact, there was actually no way to get paid (outside of an act of congress – literally!) due to a near complete lack of payment codes for new behaviors these new care channels create. The article’s summary conclusion baldly states, “The status quo (of fee-for-service payment) isn’t viable.”
Well that takes a bit of oxygen out of the CPT, Coding, and “revenue cycle management” room!
Technology enables new behaviors, and these new behaviors will need to find new pricing models if they are to be sustainable. We have long promoted—and these authors seem to agree—that virtual capabilities will soon be recognized not as something new, but rather as just another channel to access care. The authors’ further comment that, “…it’s clear that neither patients nor physicians want to go back to a world in which in-person visits are the only form of care delivery. Instead, they want the ability to choose among various options on the continuum of modes of interaction—from in-person visits to video visits to asynchronous messages—to select the mode that best fits their clinical needs and personal preferences.”
We couldn’t agree more.
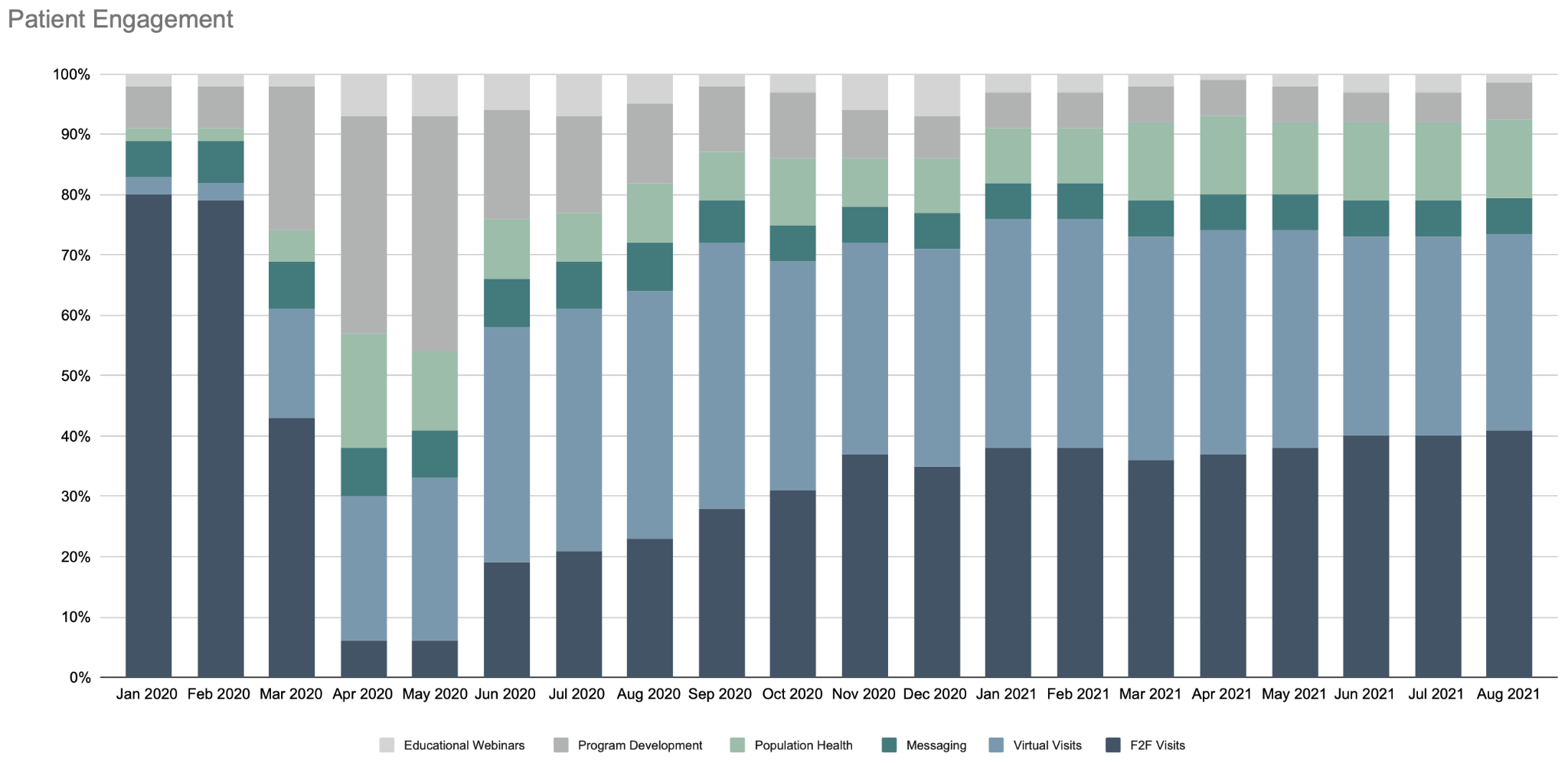
In fact, we have previously described this notion of Care is Care, but Care is Not Fungible. We believe that the care channel should be seamless to the member but that the member needs to be aware of what type of care they are actually getting. A 10-minute video consultation or a string of chatbot messages is not equivalent to an ongoing relationship with a care team that knows you personally, provides comprehensive and connected care services, and is accountable for your health outcomes. I believe this relationship-based, goal-directed care model is vastly superior to transactional care, particularly when the convenience, access, and experience is also better. This is why we see our members settling into a natural equilibrium of 40% in person, 40% online, and 20% population heath and condition-specific programming (see below) while the industry as a whole is trending back down to below 10% utilization of virtual care.
The difference between the experience we deliver at Crossover and the experience that others deliver seems to be pegged back to the pernicious presence of fee-for-service. The authors claim it is an “important obstacle” standing in the way of healthcare achieving the vision of a natural hybrid approach to care delivery (for us, this vision is a reality!). I’d argue that it’s not just “an” obstacle—it is the obstacle. Are there other sectors in which the business model of the service forces the customer to engage in only one way? If there are new technologies driving new customer behaviors (an obvious willingness to engage in the multi-channel and choice-driven health care service), wouldn’t it follow that new payment models should adapt as well?
The authors quite succinctly encapsulate the transactional nature of traditional health delivery into the phrase “units of care.” It’s a great, though damning, way to describe the fixation on volume in healthcare. You don’t get compensated for how much healthier your population is becoming—it’s simply, “How many units did you process today?” Yes, you, the patient, are a “unit” and the reductionist thinking by its very structure prevents both a holistic as well as an empathetic view of care. Worse still is the indication that health systems and payers—facing the complexity of new tech-enabled consumer behaviors as well as emerging multi-channel care optionality—are simply throwing their hands up and telling providers and patients that they’re going back to their old ways. The authors conclude with a definitive, “Only a payment system that encompasses some form of capitation will eliminate these issues.”
At Crossover, we are seeing and experiencing many of the challenges the article describes, as we introduce new forms of virtual care delivery while simultaneously moving to more forms of capitation, risk-sharing, and outcomes-based payments. The point of moving to more capitated-like models is not to enable virtual care (consumers will demand this on their own), but to enable new payment approaches to care delivery in general, as these just don’t fit cleanly into historical fee-for-service. This is particularly important at Crossover because we incorporate digital tools as an integral but not defining part of the care experience, focus on whole health and not just sickness, encompass the whole patient journey including referrals, and already innovate with other complementary services that can now be deployed and paid for under value based arrangements. .
The authors write that the switch to new payment models is “hard work”. However, from our experience at Crossover, it is the hard work that moves you up the mountain, as well as what helps you appreciate the view. And, it’s only for those willing to put forward that hard work, that obtaining the value-based vista becomes…inevitable!


Leave a Reply