

Value-Based Care: The Latest Virtue Signaling in Care Delivery
About two years ago, I started hearing quite a bit about Social Determinants of Health, Health Equity, and Health Disparities. At first, I welcomed the new terms as they describe a very long-standing but newly recognized issue. I felt the world was finally waking up to the fact that so much of our health is related to our zip code as opposed to a billing code). Soon, a growing number of conferences dedicated time to these topics and the traditional “I support the next thing” crowd piled on. However, although I do continue to hear more and more about these very challenging structural and societal issues and healthcare’s central role in mitigating them, I’m seeing few solutions being implemented that actually tackle them. Furthermore, most of what I do see is somehow wrapped up in the development of “Value-Based Care” mechanisms where the main part of the discussion is the “upside and downside” risk assumed by the provider group.
True Value-Based Care as delivered by care providers will have to embrace these larger societal needs to succeed in positively shifting health access, status, and costs across our communities. However, the thorny issue of how all the “new work” required to actually impact these issues gets paid for remains, well, a thorny issue. And, there is a comprehensive new body of work that must be done which necessitates a comprehensive new approach to payment as well.
How are all of those open care gaps actually tracked? Who is taking those insights and actually delivering them to patients through new channels? How are those new channels developed? What technology is being deployed? Who is actually engaging with the community to look beyond the medical determinants? What about the cost to develop the health programming that delivers the educational content and ensures it is useful? What about the marketing, the acquisition efforts, and helping members truly engage in their health? How is the engagement capability developed and improved? What about your data science team, your software engineers, and your health outcomes experts? What about all the other overhead to run and operate a business, to hire, staff, and train your team, to operate your finances, to have rock solid accounting, to get your sales and account management teams online?
Old financial models and perceptions of the role of primary care simply won’t work, as much as entities continue to try to develop value-based models with old tools. Straining at the 5% primary care spending gnat while swallowing the other 95% secondary care spending camel remains just an incredible irony to me. It turns out the new wine of Value-Based Care doesn’t fit so well into the proverbial old bottle of Fee For Service paradigm.
There is a clear path forward—pay “more and different” for Primary Health. However, this path requires that you are able to hold two insights simultaneously in order to “see” the way forward: 1) expect to reallocate MORE spending to primary care than you do today; and, 2) simultaneously expect to spend LESS on your total cost of care. Just comparing your primary care spend year over year is problematic—you are likely not spending enough today.
To make this more tangible, let’s look at a simple visual using a baseline $1 of healthcare spend:
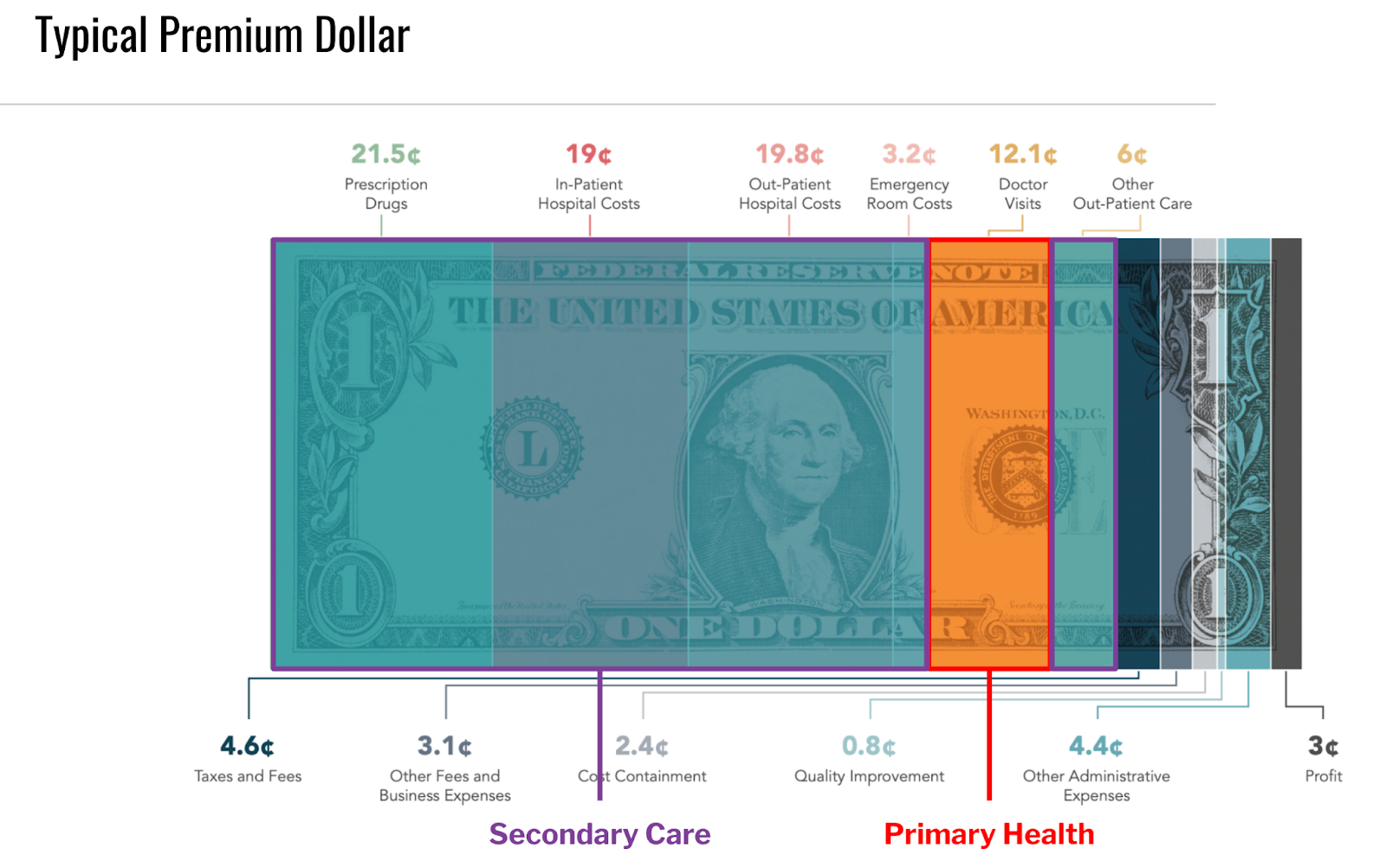
What needs to happen is this: The typical 5-7% being spent on Primary Health needs to increase to 10-12%. This simple reallocation moves money away from the (in many cases) unnecessarily high-cost secondary care and puts it into much lower cost, higher impact, and more value added Primary Health. Of note, interesting case studies can be found in both Rhode Island and Oregon where they legislatively achieved these higher investments in primary care and reduction in overall costs over a period of a few years. I personally would like to see market mechanisms recognize the true value of primary care and see payers voluntarily choose to fund Primary Health at twice the rate it is today in order to reduce overall costs in that ~15% zone (which we consistently see at Crossover). This subtle shifting of a small fraction of secondary care spending into Primary Health can produce sizable overall healthcare spending reductions. It’s a simple concept and one that has ever hardening concrete evidence.
If you are an employer seeking to implement “Value-Based Care,” I hope you’re serious about it. You should be addressing foundational issues like SDoH, prevention and screenings, and health disparities for your employees, and you can’t accomplish that if your primary objective is to drive costs out of your primary care spend, rather than out of your overall health spend. As noted previously from Implementing High-Quality Primary Care (pg 7):
“The relatively small proportion of health care expenses spent on primary care today becomes an opportunity. A small absolute increase in primary care spending, redistributed from the large expenses across the rest of the system, can have a high proportional effect on primary care and work to stabilize the health system overall.”
For consultants helping employers to make the move to VBC—you should know better than to expect “more and different” levels of care, outcomes, and impact on the total cost of care if you revert back to the dead end of transactional fee for service as your comparative unit of account. This is inaccurate and not helpful to your clients. You know unit costs don’t translate into the new models of care that are both expected and being proven to have impact. Instead you should use your influence and expertise to guide them to the forefront of spending adequately on Primary Health with the expectation that it pulls down the total cost of care.
It’s not hard to understand, but I understand it’s hard to reach a shared understanding on this concept: “Primary Health is the only health care component where an increased supply is associated with better population health and more equitable outcomes. For this reason, primary care is a common good, making the strength and quality of the country’s primary care services a public concern.” Despite any obstacles, we can and must move beyond virtue signaling to instead signal the virtuous path forward toward “health as it should be.”


Leave a Reply