

Interview: Nate Murray, Part 2 – Proving our Model, Again
This is the second of two posts (Part 1 is here) where we speak to Nate Murray, co-founder of Crossover Health, alongside Scott Shreeve, MD and Rich Patragnoni, MD. Nate talks about Crossover’s big switch to digital and the role of the pandemic in supercharging this transition.
What’s the Value Proposition you put in front of clients, now that you have history, evidence, and a book of business?
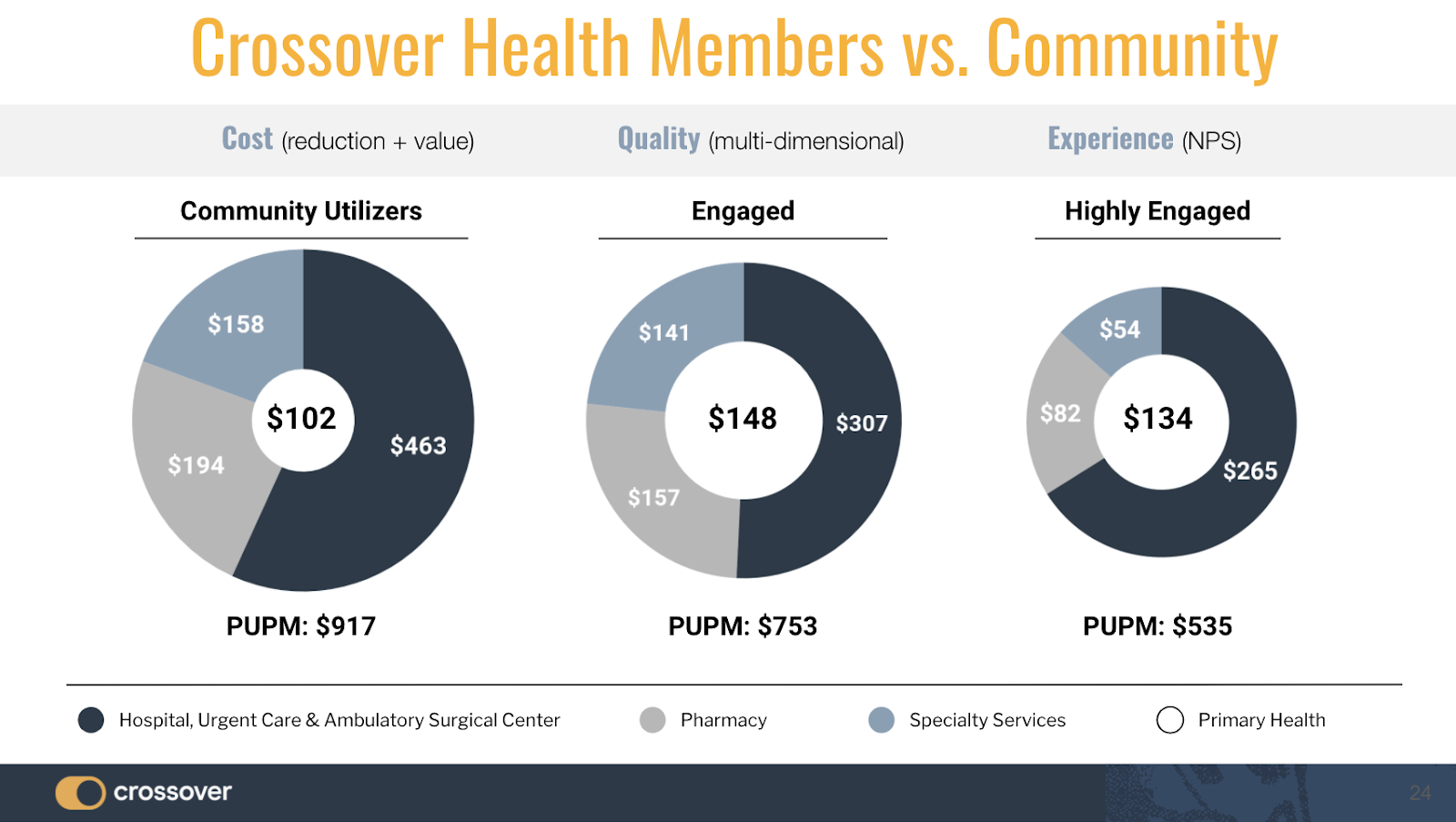
It hasn’t changed that much. We always think about how we should solve the problem of healthcare. Remember those concentric circles from our earliest days, when the inner primary care circle was small and the overall system spend was bigger? I was talking to a client about this image and said “I’ve been showing you this image since 2012. Now it’s 2020, and I’m pleased to report we can replicate this image for you, where you’ve increased spend on primary care and decreased spend in the outer circle.” This vision—that we aspired to and said was the problem to solve in healthcare—is what we’ve been able to accomplish at this company. So our message to clients is, “Get the primary care doctor closer to the patient. Get all the wedges that have been placed in there by the insurance companies and health systems out of the way, and just let a patient and provider solve the problem.”
While what we’ve done to date is great, we have run into limitations with the physical center when it comes to getting care to everyone, so the biggest change is our pivot to Digital First. As Scott, Rich, Jay, and everyone else is saying, the care model is going to stay the same. It’s now just the combination of physical and digital. That’s the nuance. I continue to wrestle with the idea of how we maintain this relationship as we move headlong into this new digital channel. That relationship, and the implied trust, is so important. Fortunately, the clients who have joined our growing national network share our vision, and believe just as fervently that traditional telemedicine simply can’t get it done.
How do you think the care model will evolve with digital?
I look at the moment we’re in today just like I do the moment before we built our first facility. People were going, “Awesome primary care? What does that mean?” Scott was talking even then about care teams, about design and experience, but we had to build that first facility to show people exactly what we meant. And the same thing is happening now—we get RFP’s that ask us to describe our telemedicine technology solution, cast in terms as if the technology is the thing. We have to politely, but bluntly state, that the technology is actually NOT the thing, the care model is the thing. Sure, the model is evolving, but at the end of the day, it’s all about a patient and a provider, and how they connect with—and without—technology.
Let me expand on that a bit because it’s an important point. We get asked, “Well how many video visits do you do?” And it’s just like the old paradigm for primary care, where 30 visits per doc per day meant you had a successful practice. It’s going to take the early adopters—the believers—to get on our care model platform to see how the model is different. This isn’t 30 simple things with a random doctor. It’s not about visits, nor volume, nor vaporware AI technology. It’s about an ongoing relationship where there might be multiple interactions to solve your healthcare situation. We view each of these as a “project” organized as an episode of care. It is a simple, ongoing, and natural communication between you and your care team, that fits into your life just like all the other great services that you use. Simple. Seamless. Satisfying.
Those three words never get strung together in a sentence describing healthcare. The reason is that typically, healthcare today is intrusive, disconnected, and to be frank, just jarring. The scheduling, the rushed appointment that breaks up your day, the lack of clarity, the blocks, the friction, and just the overall annoyance. We see our model as being really simple—an easy relationship that fits into your everyday life. But just as with our first clinics, I don’t think we’re going to be able to talk our way through that story—people need to touch, feel, and experience it to truly understand.
We’re fortunate that we have always had—and continue to have—several first movers—partners that now have 8-10 years of experience working with us. During that time span, we have demonstrated again and again that we are leading them to a new healthcare future, so they remain willing to dive into the deep end of the pool with us into new areas of care. And, they are really seeing that this is not just an extension of the care in our physical centers, but rather a foundational shift in how care will be provided in the future. It’s been awesome.
Would you consider that the pandemic has given Crossover the “license” to pivot to digital first?
Both Jay Parkinson, MD our Chief Designer, and Scott have been talking about how “we are all remote now.” What we thought would take 3-4 years actually happened in 3-4 weeks. It has taken something as serious as the pandemic to drive this change. People haven’t really felt comfortable with virtual care just quite yet and then—suddenly—access to physical care was taken away, and people said, “Okay, now I need this thing.”
Then, the patient uses telemedicine and realizes that to describe their symptoms they don’t actually need to look at the provider on a Zoom call or use a video visit. In fact, just like everyday life, describing issues in texts and messages is actually better for them, and that realization allows us to move beyond the old paradigms, and past the old channels. Something else we’ve seen—in both in person as well as virtual visits—people are usually so focused on the time. Whether it’s the standard 8-12 minutes most people get now or our more generous 30-minute visits, time always seems to be the focus. People are often so worried about whether they forgot to ask something, or can’t recall everything the doctor said to do.All of these time-bound pressures go away when the conversation is continuous—before, during, and after the visits—because the communication itself becomes the documentation.
This is so different than just taking the visit and digitizing it. For example, digitized urgent care doesn’t work in the telemedicine construct—all it does is convert the waiting room from a physical nightmare to now a digital one, which I find to be unimaginative and disappointing. The whole point of the technology is to leverage its capabilities—not just its efficiencies. There is new capacity for both members and providers in how they communicate, what is recorded, and what can be accomplished when an open, ongoing channel exists. We shouldn’t settle for a Radio with Pictures paradigm.
Looking at COVID-19, how do you communicate ongoing value when so much of healthcare simply isn’t happening right now?
Businesses are looking at costs everywhere, and putting pressure on reducing them, including in healthcare. But one of the things I like about healthcare is that even in these times, people still need it. The business has built-in resiliency and is a bit more resistant to economic cycles.
One of the biggest challenges for us in this cost-cutting time, however, is that we’re put in the wrong bucket. We’re providers, but sometimes we’re put in client budget columns beside services like Livongo, or a wellness app, which require all kinds of approvals, and therefore are subject to all kinds of scrutiny. This is unfortunate—and to be candid, is an unfair disadvantage to us—because the providers in the community have zero scrutiny whatsoever. They go through no RFP process, they don’t have to demonstrate their value, pass security or privacy audits, endure a brutal budget approval process—and they don’t have to handle client complaints when things don’t go well for members. Nothing. Nada. Zip. They just send in the bills and count the money as it comes in. This is why we keep pushing our employers to take this service out of their wellness budgets, and instead pay for it directly from their self-funded accounts, which are reserved to pay doctors.. Some employers get this, but many do not, and this will be a big area of focus for us in the years ahead.
As you move to new care delivery models, what’s your view on the sharing of risk?
Risk-sharing makes a lot of sense, in general. However, in the commercial space (non-medicare and non-medicaid) it struggles because all of the existing models for risk-sharing are based on a system of super low primary care utilization. The companies that create these risk models find it hard to contemplate the kind of primary care utilization we deliver, and in spite of data showing that well-funded primary care delivers and offsets spend elsewhere, these companies have to make a leap of faith into a world with much higher primary care use.
The opportunity for us, like everything else, is to go directly to an employer that’s willing to take the risk approach, likely as primary care unbundled from the system. The employer will pay a more substantial fixed fee for primary care, but then should immediately start to observe what effect it has on the rest of the healthcare spend.
I hate to use the term HMO (which still feels like a dirty word), but to be honest, the capitation concept is actually what works if the providers can innovate and deliver value underneath the budget created. If you look at historic models, however, the primary care fixed fee is really, really low. It needs to be higher to support the advanced primary care we deliver; it is this care that produces the large downstream impact on costs. That shift in perspective is challenging for any entity that’s paying healthcare costs until they spend the time to really analyze their spend, realign their priorities and where they will invest, and then set up the systems and capabilities to measure impact. Until an employer is willing and able to do this, they are flying blind—just writing checks each month for low quality, low value care.
Where do you see the company in a couple of years?
I believe that this idea of “unbundled” primary care that we’ve been working towards is going to take hold. Labeling it is something that we’ve been working on for the last six months, but doing it has been part of the company for a long time. I want people to see that a “platform” of primary care is an essential benefit and a way to think about benefit plan design at a national level. We’ve always been a bit limited by the physical building. With digital access to care anywhere, we can now promote this concept of unbundling primary care from traditional health insurance and treating it more like a membership that people join, with navigation back into the secondary care system when needed. That’s how we’ll change the expense equation of healthcare across the country.
We’ve used unbundling in a couple of informal settings with employers, and it has only partially landed. It reminds me a little bit of when we introduced nearsite as a concept. People kind of understand it but not really—it leaves them a little confused. They really like the idea of disconnecting this core thing (primary care) from everything else, and making sure this core thing is everywhere. So I can see the word “unbundled” evolving, but not the concept. It’s a reflection of what we do and what we think our future is.
One of the areas we are starting to see employers connect with the idea of unbundled primary care is in their benefit plan design. Employers are realizing that the greatest savings happen when their members use Crossover for ALL their primary care services and Crossover is able to deliver advanced primary care. To encourage this behavior, employers are starting to structure plan designs around Crossover Health with a lower premium and richer benefit to encourage use. We are excited to have these attributed members and continue to demonstrate that the pathway to improve healthcare is a greater investment in primary care.
If you were not at Crossover, what would you be doing?
That is a great question . . . on a personal level, if I had more time I think I would be spending it coaching my boys in youth sports. We are a total sports family. A perfect Saturday for my wife and I is back to back games all day! We can’t get enough of it. I was coaching my 4 year old son’s tee ball team this spring and we were totally crushed that the season was cancelled because of Covid-19. It was a total blast playing baseball with these little dudes that could barely catch a baseball. The best part of the team was watching the players warm up to this playlist!
Many thanks to Peter Heywood (one of our long-standing brand advisors and business consultants) who helped conduct these interviews.


Leave a Reply