

We are all remote now
As I wrote in my prior post, we have been ramping into a 24/7, every waking moment, COVID-19 response since early March. While the warning signs and extreme measures taken in China seemed overly authoritarian, I think the Italian response and serialized shutdowns were a big wakeup call here in America. The crowd that was recently claiming “this is just the flu” has been feeling some real and palpable shock. School shutdowns, forced “Sheltering in Place,” and a variety of other measures that just two weeks ago would have been the thing of survivalist and prepper lore, are now with us.
We are all remote now.
We have been talking about a transition to a digital first future in healthcare for some time, which will mirror what is happening in society in general. We’ve spoken about it in the context of a gradual introduction of the new technology, getting people more comfortable with the tech-enabled interactions, and perhaps most importantly, what is now possible with the introduction of asynchronous care. At Crossover, we have already moved well past video visits into something totally new —bolstered by anytime, asynchronous access to the care team that you have built a consistent relationship with by investing your time, information, and energy. Your team, with your permission, has access to your personal information, is gathering your claims data, and in partnership with you, is providing meaningful, timely, and relevant care insights.
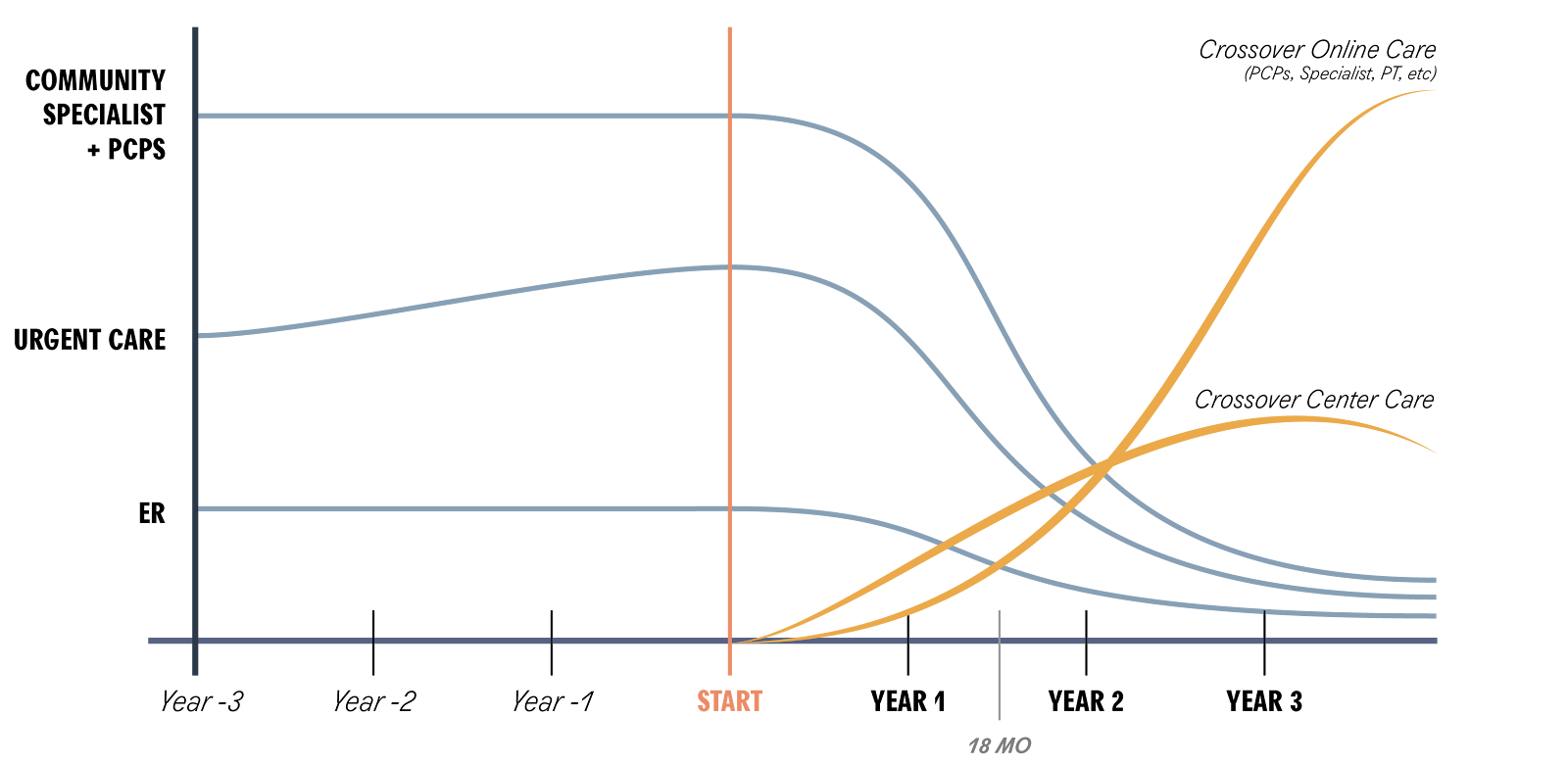
We also see all kinds of possibilities with the asynchronous approach—time dilation and new methods of value creation—as well as significant efficiencies and better ways to deliver outsized outcomes. We understood early on that this new model would fundamentally shift the way that people would use our current physical center service offerings as illustrated in the sketch below:
What we didn’t anticipate was the Black Swan tsunami that came in the form of COVID-19. A novel new virus, just 100 nano microns big, has created trillions of dollars of dislocation in the global economy at an unprecedented scale and scope. It is effectively forcing people to rethink how they live every aspect of their lives, how they communicate, coordinate, and connect with their fellow humans in order to #stopthespread and #flattenthecurve. Not only is the technology to be remote widely available now (as is the required high-bandwidth infrastructure needed to enable this), but it has become literally required. You can’t access certain things any other way now, including even in healthcare.
As the graph above shows, we always knew the day would come when digital would eclipse our physical services—we just didn’t see the transition happening within a two week period. Underpinned by the need to respond to this health crisis, we have effectively skipped YEARS of slow, grinding adoption, dodging multiple rounds of presentations, RFP’s, ROI analyses, adoption rate comparisons, and trying to piece together value statements on the service. All gone. All done. All unnecessary. In one swoop—by fate and soon by fiat—we are all remote now.
The incredible speed of the switch, along with the urgency, both present a challenge. I think we will compound the tragedy that is currently unfolding if we simply apply new technology to old ways of doing things. Even now, we are starting to see people excitedly (albeit inaccurately) talk about Virtual Health like it is a brand new thing (@realdonaldtrump —telehealth is not a “wonderful new invention”) or a near perfect solution. Our own Jay Parkinson, MD has called out the emerging opportunity for Virtual Care to truly transform how healthcare is understood and experienced. As he points out, virtual or remote interactions can’t just be a sloppy application of videos to the old transactional “visit” framework. All of it—telehealth, virtual visits, remote care, digital first—can be (and must be) so much more. Providing ready access, continuity of care, and connectivity to a much greater degree than traditional in-person care, is necessary for our COVID-19 response now, and desirable later.
Our all-consuming focus has to be getting through this crisis by offering our current services remotely. However, let’s not lose sight of the singular opportunity to expose to everyone what is possible in how we deliver care, and the potential and promise of the new digital model of care delivery to fundamentally rearchitect the care relationship.


Pingback: Pandemic Primary Care – Scott Shreeve, MD